
Hypoplastic Left Heart Syndrome
What is hypoplastic left heart syndrome?
Hypoplastic left heart syndrome (HLHS) is a combination of several abnormalities of the heart and great blood vessels. It is a congenital (present at birth) syndrome, meaning that the heart defects occur due to underdevelopment of sections of the fetal heart starting during the first eight weeks of pregnancy.
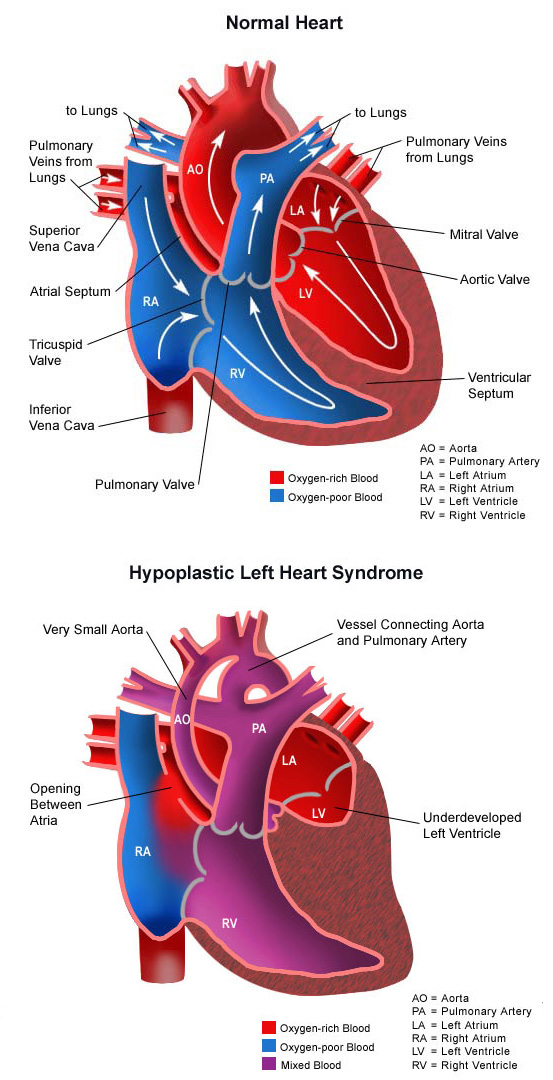
In the normal heart, oxygen-poor (blue) blood returns to the right atrium from the body, travels to the right ventricle, then is pumped through the pulmonary artery into the lungs where it receives oxygen. Oxygen-rich (red) blood returns to the left atrium from the lungs, passes into the left ventricle and then is pumped out to the body through the aorta.
In hypoplastic left heart syndrome, most of the structures on the left side of the heart are small and underdeveloped. The degree of underdevelopment differs from child to child. The structures affected usually include the following:
- Mitral valve. The valve that controls blood flow between the left atrium and left ventricle in the heart.
- Left ventricle. The lower left-hand chamber of the heart. It receives oxygen-rich (red) blood from the left atrium and pumps it into the aorta, which takes the blood to the body. The left ventricle must be well-developed, strong, and muscular in order to pump enough blood to the body to meet its requirements.
- Aortic valve. The valve that regulates blood flow from the heart into the aorta.
- Aorta. The largest artery in the body and the primary blood vessel leading from the heart to the body.
Perhaps the most critical defect in HLHS is the small, underdeveloped left ventricle. This chamber is normally very strong and muscular so it can pump blood to the body. When the chamber is small and poorly developed, it will not function effectively and can’t provide enough blood flow to meet the body’s needs. For this reason, an infant with hypoplastic left heart syndrome will not live long without surgical intervention.
What causes hypoplastic left heart syndrome?
Some congenital heart defects may be due to a genetic defect that causes heart problems to occur more often in certain families. In hypoplastic left heart syndrome, there may be abnormalities of other organs.
In many children, HLHS occurs by chance, with no clear reason for its development.
What are the symptoms of hypoplastic left heart syndrome?
Infants with HLHS usually develop symptoms shortly after birth. However, each child may experience symptoms differently. Symptoms may include:
- Cyanosis (blue color of the skin, lips and nailbeds)
- Pale skin
- Sweaty or clammy skin
- Cool skin
- Heavy and/or rapid breathing
- Fast heart rate
- Cold feet, diminished pulses in the feet.
The symptoms of hypoplastic left heart syndrome may look like other medical conditions and heart problems, and will be diagnosed by the child’s health care team.
How is hypoplastic left heart syndrome diagnosed?
In many cases, hypoplastic left heart syndrome is diagnosed while the fetus is still in the womb. After birth, the child’s parents or doctor may find the baby to be listless, breathing rapidly or cyanotic (blue).
A pediatric cardiologist specializes in the diagnosis and medical management of congenital heart defects, as well as heart problems that may develop later in childhood. The cardiologist will examine the child, listen to the heart and lungs, and make other observations that help in the diagnosis. Diagnostic testing for congenital heart disease varies by the child’s age and clinical condition. At CHOC, our specialists may use one or more of the following diagnostic tests to diagnose a child’s heart defect:
What is the treatment for hypoplastic left heart syndrome?
Infants with hypoplastic left heart syndrome are admitted to the NICU or CVICU. Initially, the child may be placed on oxygen, and possibly even on a ventilator, to assist with breathing. Intravenous (IV) medications may be given to help the heart and lungs function more efficiently. Staged surgery repair is usually the treatment of choice for HLHS.
- Stage 1: Norwood procedure. The first operation takes place shortly after birth and serves to make the right ventricle the main pumping chamber for blood flow to the body. The outflow from the right ventricle (the pulmonary artery) and the outflow from the left ventricle (the aorta) are connected side-by-side in order to allow all blood from either the right or left ventricles to reach the body. A connection (shunt) is also made to make a pathway for blood to flow into the lungs to receive oxygen. Following this operation, the infant will still have cyanosis since oxygen-poor (blue) blood from the right atrium and oxygen-rich (red) blood from the left side of the heart mix and flow through the aorta to the body.
- Stage 2: Glenn shunt. The second operation takes place at about 4 to 6 months of age and replaces the shunt supplying blood flow to the lungs with another connection to the pulmonary artery. In this operation, the shunt is removed, and the superior vena cava (the large vein that brings oxygen-poor blood from the head and arms back to the heart) is connected to the right pulmonary artery. Blood from the head and arms then passively flows into the pulmonary artery and lungs to receive oxygen. However, oxygen-poor (blue) blood returning to the heart from the lower body through the inferior vena cava will still mix with oxygen-rich (red) blood in the left heart and travel to the body, so the child will remain cyanotic. This operation helps create some of the connections necessary for the final operation, the Fontan procedure.
- Stage 3: Fontan procedure. This operation takes place at about 2 to 3 years of age and allows all the oxygen-poor (blue) blood returning to the heart to flow into the pulmonary artery and lungs, greatly improving the oxygenation of the blood. The Glenn shunt, connecting the superior vena cava to the right pulmonary artery, is left in place. A second connection is made directing blood from the inferior vena cava to the right pulmonary artery as well. This connection can be created in slightly different variations, depending on the method child’s surgeon prefers, and what is best for the child.
Learn more about heart surgery at CHOC.
What is the postoperative care for a child after surgery?
After surgery, infants will return to the CVICU to be closely watched during recovery. While the child is in the CVICU, special equipment will be used to help him or her recover, and may include the following:
- Ventilator. A machine that helps the child breathe while he or she is under anesthesia during the operation. A small, plastic tube is guided into the windpipe and attached to the ventilator, which breathes for the child while he or she is too sleepy to breathe effectively. After a HLHS operation, children will usually benefit from remaining on the ventilator for at least a few days.
- Intravenous (IV) catheters. Small, plastic tubes inserted through the skin into blood vessels to provide IV fluids and important medicines that help the child recover from the operation.
- Arterial line. A specialized IV placed in the wrist or other area of the body where a pulse can be felt, that measures blood pressure continuously during surgery and while the child is in the CVICU.
- Nasogastric (NG) tube. A small, flexible tube that keeps the stomach drained of acid and gas bubbles that may build up during surgery.
- Urinary catheter. A small, flexible tube that allows urine to drain out of the bladder and measures how much urine the body makes. This helps determine how well the heart is functioning. Immediately after surgery, the heart will be a little weaker than it was before, and the body may start to hold onto fluid, causing swelling and puffiness. Diuretics may be given to help the kidneys to remove excess fluid from the body.
- Chest tube. A drainage tube will be inserted to keep the chest free of blood that would otherwise accumulate after the incision is closed. Bleeding may occur for several hours, or even a few days after surgery.
- Heart monitor. A machine that constantly displays a picture of the child’s heart rhythm, and monitors heart rate, blood pressure and other values.
Additional equipment not mentioned here may be required to support the child after surgery. The hospital staff will explain all of the necessary equipment.
Occasionally, the chest may be left open for the first few days, and covered with a special bandage. The open chest prevents compression of the heart by the rib cage. The chest is then closed several days later after the swelling in the chest has gone down and the heart has had a chance to adjust to the new circulation.
Children are kept as comfortable as possible with several different medications—some that relieve pain and some that relieve anxiety. The staff will also be asking for the family’s input on how best to soothe and comfort the child.
As the baby recovers from surgery, the staff will provide instructions regarding medications, activity limitations, and follow-up appointments before the child is discharged.
Infants who spent a lot of time on a ventilator, or who were fairly ill prior to surgery, may have trouble feeding initially. These babies may have an oral aversion; they might equate something placed in the mouth, such as a pacifier or bottle, with a less pleasant sensation, such as being on the ventilator. Some infants are just tired, and need to build their strength up before they will be able to learn to bottle-feed. Strategies used to help infants with nutrition include the following:
- High-calorie formula or breast milk. Special nutritional supplements may be added to formula or pumped breast milk to increase the number of calories in each ounce, thereby allowing your baby to drink less and still consume enough calories to grow.
- Supplemental tube feedings. Feedings given through a small, flexible tube that passes through the nose, down the esophagus, and into the stomach, that can either supplement or take the place of bottle-feedings. Infants who can drink part of their bottle, but not all, may be fed the remainder through the feeding tube. Infants who are too tired to bottle-feed at all may receive their formula or breast milk through the feeding tube alone.
- Gastronomy tube. Occasionally, a more permanent feeding tube, called a gastrostomy or G-tube, is necessary to ensure that the baby takes in enough calories to grow and gain weight.
How is a child cared for at home after hypoplastic left heart syndrome surgical repair?
Pain medications, such as acetaminophen or ibuprofen, may be recommended to keep the child comfortable at home. The child’s doctor will discuss pain control before the child is discharged from the hospital.
If any special treatments are to be given at home, the nursing staff will ensure that family members are able to provide them, or a home health agency may assist.
Families may receive additional instructions from the child’s health care team.
What is the long-term outlook for hypoplastic left heart syndrome?
Hypoplastic left heart syndrome is a very serious congenital heart defect, and infants and children who have the staged surgical procedures will require special care and treatment to support growth and nutrition. These children may have diminished physical strength as well as slowed developmental progress and may need support. Regular visits with the child’s cardiologist are crucial to monitor the child’s progress and to support his or her health. Medications may be necessary to maintain the child’s level of health. The child’s cardiologist will provide you with ongoing, regular information regarding the child’s specific prognosis and health care needs.