
When a child is diagnosed with a medical condition, many parents feel overwhelmed with questions. Whether your child has been recently diagnosed with hypospadias, will soon be undergoing corrective surgery for the defect or needs further treatment due to complications from a procedure performed at another hospital, it is important to know as much as possible as your family makes important decisions about the child’s care.
What is hypospadias?
Hypospadias is a condition that affects the urethra and the foreskin on a male’s penis. The urethra is the tube that carries urine from the bladder to the outside the body. Hypospadias is a disorder in which the male urethral opening is not located at the tip of the penis.
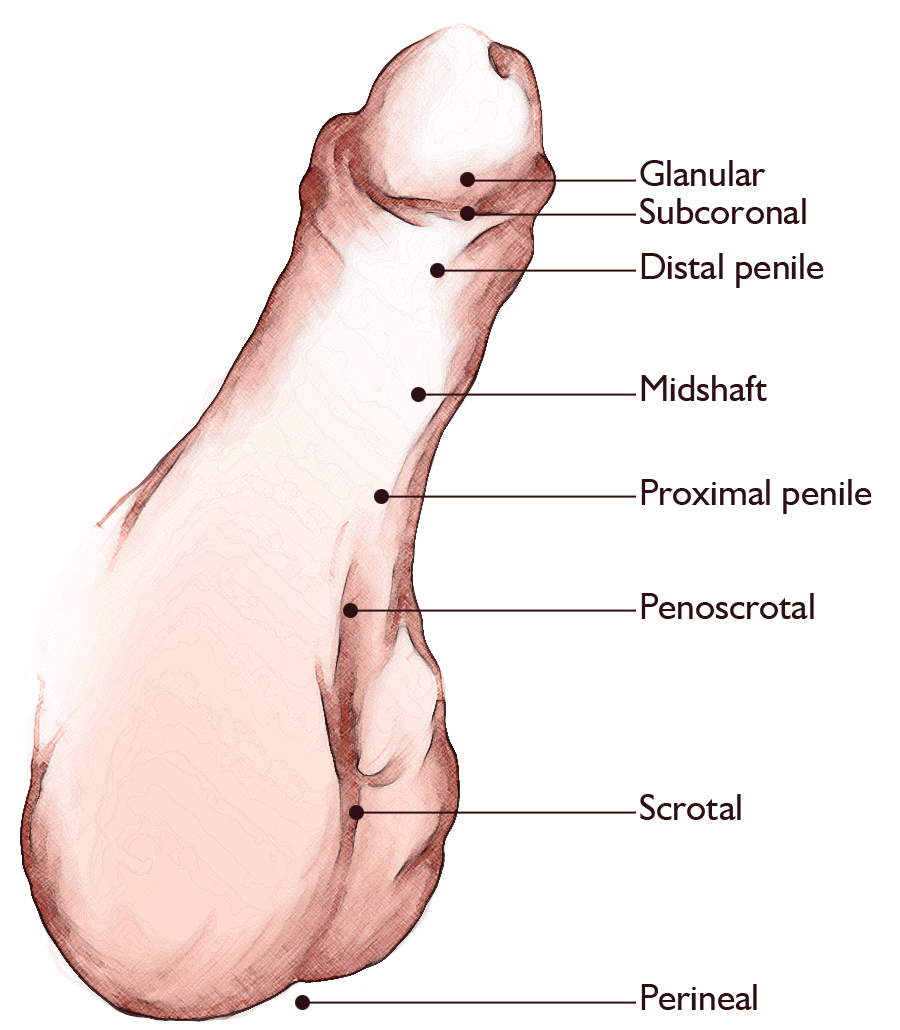
Most commonly with hypospadias, the opening is located along the underside of the penis close to the tip, but can be located anywhere along the urethra all the way down into the scrotum.
What causes hypospadias?
The cause of hypospadias is still unknown. Hypospadias is a condition that is present at birth and is the result of incomplete development of the urethra. Commonly seen with hypospadias is incomplete development of the foreskin. This typically is noted with extra foreskin on the top side of the penis and no foreskin on the underside of the penis. This incomplete development of the foreskin may also be referred to as “hooded foreskin.”
Who is affected by hypospadias?
According to studies:
- Hypospadias does have a genetic component, and sons of men with hypospadias do have a higher risk of having it as well
- Prematurity and low birth weight are also considered risk factors for hypospadias
What are the symptoms of hypospadias?
The following are the most common signs of hypospadias:
- Abnormal appearance of foreskin and penis on exam
- Abnormal direction of urine stream
- The end of the penis may be curved downward (chordee)
The signs of a hypospadias may resemble other conditions or medical problems. Through careful examination, the CHOC Urology Center specialists rule out other conditions before making the hypospadias diagnosis.
How is hypospadias diagnosed?
A health care professional usually diagnoses hypospadias at birth and can be identified with a physical examination. It is important to not circumcise a child with suspected hypospadias until he has been seen by a pediatric urology health provider.
Learn more about making an appointment with a CHOC Urology Center pediatric urology specialist.
How is hypospadias treated?
Mild forms of hypospadias may not require any intervention. If a hypospadias is more severe, surgical correction may be recommended. If left unrepaired, the following complications may occur as the child grows and matures:
• The urine stream may be abnormal. The stream may point in the direction of the opening or it may spread out and spray in multiple directions. It may also cause the stream to shoot directly downwards, towards the boy’s feet or body.
• The penis may curve as your baby grows causing sexual dysfunction later in life, resulting in a condition called chordee.
• If the urethral opening is close to the scrotum or perineum, the child may have problems with fertility later in life.
Specific treatment for hypospadias will be determined by your baby’s health provider based on:
• The child’s gestational age, overall health and medical history.
• The extent of the condition.
• The baby’s tolerance for specific medications, procedures or therapies.
• Expectations for the course of the condition.
• The family’s opinion or preference.
Not all hypospadias defects will need to be repaired, which will be determined with the child’s health provider and family. If the hypospadias needs surgical repair, it is usually done when the baby is between 6 and 24 months, when penile growth is minimal. At birth, the child should not be able to undergo circumcision, as the extra foreskin may be needed for the surgical repair. The surgical repair can usually be done on an outpatient basis (and may require multiple surgeries depending on the severity).
What is the long-term outlook for hypospadias?
At the CHOC Urology Center, we follow our patients throughout childhood by checking their urine flow rates and post urination residual measurements to ensure that the urine is flowing and emptying the body as it should.
Although rare, strictures or fistulas can develop after the hypospadias repair has been made. These are either “leaks” where a second hole develops along the site repaired (fistula) or an area within the urethra that scars and tightens causing a stricture. Signs that a stricture has developed include urinary tract infections, straining to urinate or feeling like one has to push or grunt to urinate.











